PKI NASH and Location Certificates Expiring 2022
PKI certificates are required by many businesses for maintaining access to digital health tools including electronic prescribing and My Health Record. Two such certificates are about to expire for some practices. These are the National Authentication Service for Health's certificate (commonly referred to as a 'NASH' certificate), and Medicare's 'Location' certificate.
o The NASH certificate provides secure transactions between your practice and My Health Record and other digital health tools. This certificate is used by MedicalDirector Helix and Clinical, and must be renewed for continued communication between these applications and My Health Record.
o The Location certificate is used for secure online claiming, amongst others functions, and is used by MedicalDirector Helix, Clinical, Pracsoft and Bluechip. This certificate must be renewed for continued communication between these applications and Medicare or My Health Record.
These changes may affect your MedicalDirector applications. In some instances, updating your practice's PKI certificates is required for continued secure communication between your MedicalDirector applications and Medicare or My Health Record. New certificates have been issued, and are available to download and install. Click here for information on renewing your Certificates.
Overview
My Health Record (previously known as 'Personally Controlled Electronic Health Record') is an Australian Government initiative to allow patient information to be accessed securely online, making it easier to share information between healthcare professionals. Further information is available at https://www.digitalhealth.gov.au/.
Clinical is compatible with the My Health Record system, allowing you to view CDA documentation that was created for the patient at another Practice (for example), as well as giving you the means to add your own patient documentation to the System, which can then be accessed by other clinicians. You can also upload prescriptions to a patient's My Health Record.
Documents managed via My Health Record are done so securely, and your Practice will require HI Signing and HI Encryption Certificates, as well as the My Health Record Certificate itself to access the System. These can be obtained via publiclearning.ehealth.gov.au after registering. Furthermore, patients who register can elect to secure their medical records with a password. Clinicians will then require this password in order to access their patient's records from the My Health Record System.
Configuring Clinical for My Health Record
In order to access the My Health Record system, and transfer patient documentation between Clinical and My Health Record, you must ensure you have configured the following:
Indicated your participation in My Health Record via the User Database.
Recorded your HPI-I number via the User Database.
Via the User Database, you can also edit your record to include the My Health Record details as you wish them to appear within the My Health Record system.
Recorded the Practice's HPI-O number via Tools > Options > Practice tab.
Recorded the Practice's Organisation type via Tools > Options > Practice tab.
Recorded the Practice's Service type via Tools > Options > Practice tab.
Imported the My Health Record Certificate via Tools > Options > PKI tab.
Imported the HI Signing Certificate via Tools > Options > PKI tab.
Imported the HI Encryption Certificate via Tools > Options > PKI tab.
If you have not configured one of the required fields, you will be prompted accordingly when you attempt to access a patient's My Health Record documents.

My Health Record requires an active Internet connection. If necessary, you can record you proxy server's settings via the Network Settings utility within MedicalDirector Maintenance. Please consult your System Administrator if you require assistance with this configuration.
Accessing the My Health Record Window
With Clinical configured correctly, you can access a patient's My Health Record documentation via the My Health Record menu within the patient's Clinical Window. You will be presented with the My Health Record window, an example of which is shown below.
Note that when you first access the My Health Record system, you will be prompted to complete your user name details. You will only be asked this once.
The 'My Health Record View' tab

The My Health Record View tab lists the patient's My Health Record documents. |
|
|
Allows you to gain access to documents that have been password-protected by the patient - it is the patient who controls access to their My Health Record documentation. Any document can be applied one of two access levels;
Click the Change/Gain Access button, and then select from the three Access Type options;
|
Button: Show Recent Shared Health Summary |
Displays the latest Shared Health Summary. This item will be disabled if there are no Shared Health Summaries to view. See Creating CDA e-Health Documents for information on creating Shared Health Summaries. |
Button: Show Medicare Records |
Retrieves MBS, PBS, AIR and ADOR records from the My Health Record System for the selected patient. |
Button: Show Medicine Records |
Retrieves prescription and dispensed records from the My Health Record System for the selected patient. |
Button: Reset All Filters |
Resets all filters applied to this tab. See Filtering Records on the My Health Record Window for more information. |
|
Hides/shows the document preview pane in the lower half of the My Health Record window. |
|
Navigate forward/backward through each page of a multi-page document. If a document consist of only one page, these buttons will be unavailable. |
|
Prints the selected document. |
|
Displays a selected document in Full Preview mode. |
|
Closes 'Full Preview' mode, and display the list of documents again. |
|
Opens Letter Writer and presents you with the New dialogue window, prompting you to select a new CDA eHealth document to create. |
|
Replaces a selected document with a more recent version from the patient's record. The two documents must be of the same CDA type. |
|
Removes a selected document from the My Health Record system. This is only available if you are the creator of the original document, or it was created by another user from the same Practice (i.e. with the same Practice HPI-O recorded via Tools > Options > Practice tab. |
|
Saves a selected document to the patient's record in Clinical. The saved document will be available on the Documents tab within the Clinical Window, or the Letters tab in the case of a letter. |










The 'Prescription and Dispense View' tab

The Prescription and Dispense View tab lists prescribed/dispensed medications that the patient has granted consent to upload to the My Health Record System. Consent is typically indicated via the Enter Dose window during the prescribing process, but can also be granted/revoked afterwards by right-clicking an item on the CurrentRx tab and clicking the My Health Record Consent entry from the menu that appears. This functionality requires that you have enable ePrescribing. To view a medication on this window; First,
expand the medication details by clicking the Secondly,
click the medication details. The script details will
be revealed
|
|
|
Allows you to gain access to documents that have been password-protected by the patient - it is the patient who controls access to their My Health Record documentation. Any document can be applied one of two access levels;
Click the Change/Gain Access button, and then select from the three Access Type options;
|
|
Groups records by;
|
|
Prints the list of prescriptions, exactly as they appear displayed in the window. This means that in order to print all details, the Expand List button should be pressed first. |
|
Hides the details of each prescription. |
|
Shows the details of each prescription. |
|
Hides/shows the document preview pane in the lower half of the My Health Record window. |
|
Displays a selected document in Full Preview mode. |
|
Closes 'Full Preview' mode, and display the list of documents again. |
|
Opens Letter Writer and presents you with the New dialogue window, prompting you to select a new CDA eHealth document to create. |
|
Saves a selected document to the patient's record in Clinical. The saved document will be available on the Documents tab within the Clinical Window, or the Letters tab in the case of a letter. Alternatively you can click the Save in MD button. |




The 'Pathology Report View' tab

|
Allows you to gain access to documents that have been password-protected by the patient - it is the patient who controls access to their My Health Record documentation. Any document can be applied one of two access levels;
Click the Change/Gain Access button, and then select from the three Access Type options;
|
|
Applies any Specimen Collection Date filter you set. |
|
Clears the Organisation filter. |
|
Hides/shows the document preview pane in the lower half of the My Health Record window. |
|
Navigate forward/backward through each page of a multi-page document. If a document consists of only one page, these buttons will be unavailable. |
|
Prints the selected document. |
|
Displays a selected document in Full Preview mode. |
|
Closes 'Full Preview' mode, and display the list of documents again. |
|
Opens Letter Writer and presents you with the New dialogue window, prompting you to select a new CDA eHealth document to create. |
|
Saves a selected document to the patient's record in Clinical. The saved document will be available on the Documents tab within the Clinical Window, or the Letters tab in the case of a letter. The result will be saved to the Results Tab. |

The 'Diagnostic Imaging Report View' tab

|
Allows you to gain access to documents that have been password-protected by the patient - it is the patient who controls access to their My Health Record documentation. Any document can be applied one of two access levels;
Click the Change/Gain Access button, and then select from the three Access Type options;
|
|
Applies any Event Date filter you set. |
|
Clears the Organisation filter. |
|
Hides/shows the document preview pane in the lower half of the My Health Record window. |
|
Navigate forward/backward through each page of a multi-page document. If a document consist of only one page, these buttons will be unavailable. |
|
Prints the selected document. |
|
Displays a selected document in Full Preview mode. |
|
Closes 'Full Preview' mode, and display the list of documents again. |
|
Opens Letter Writer and presents you with the New dialogue window, prompting you to select a new CDA eHealth document to create. |
|
Saves a selected document to the patient's record in Clinical. The saved document will be available on the Documents tab within the Clinical Window, or the Letters tab in the case of a letter. |
Filtering Records on the My Health Record Window
Select the My Health Record View tab. Filtering of documents is available only to this tab.
Locate
and click  at the top
of the column you wish to apply a filter to. The filter window
appears, and example of which is shown following.
at the top
of the column you wish to apply a filter to. The filter window
appears, and example of which is shown following.
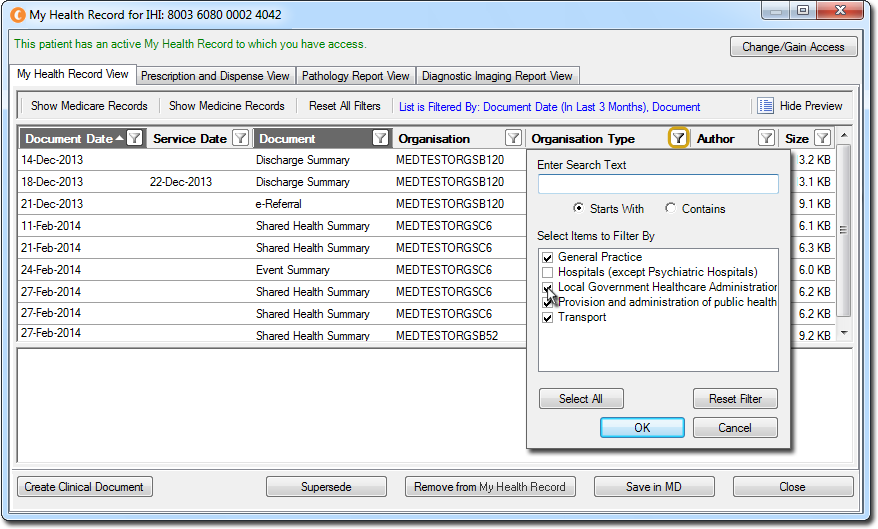
The criteria available to the filter window varies depending on
the data format and types of entries within the column you are
applying a filter to, with the example above displaying all the
types of Organisation associated with the current set of documents
in the My Health Record window.
Apply a filter;
Filter the list of documents to either start with or contain a specific term by typing the term into the Enter Search Text field, and selecting either the 'Starts With' or 'Contains' condition.
Filter the list of documents by one or more specific entries by ticking/un-ticking available options in the Select Items to Filter By list. Deselect/Select the entire list by clicking the Deselect All/Select All button (this button is a toggle). The example above will display all records where the Organisation Type is either 'General Practice' or 'Transport'.
Click the Reset Filter to reset this column's filter, closing the filter window, and returning you to the My Health Record window.
Click
 to apply your chosen filter settings to
this column.
to apply your chosen filter settings to
this column.
Downloading Documents from the Patient's My Health Record
Within the patient's record, select the My Health Record menu. You will be presented with the My Health Record window.
Locate and select the document you wish to download.
Click

If the document is of type 'Shared Health Summary' or 'Event Summary' it is saved to the Documents tab of the patient record. Documents of type 'e-Referral' or 'Specialist Letter' are saved to the Letters tab.
If the document already exists in the patient's record (it has already been downloaded from My Health Record), you will be notified accordingly.
If the document already exists in the patient's record, but on the My Health Record system there is a newer version of it, the document will be downloaded to the patient's record, and the older version will be retained within the patient's record for historical purposes.
The 'My Health Record Status' and 'My Health Record Activity Date' columns within the Documents/Letters tabs will indicate the selected document's My Health Record status, such as 'Uploaded', 'Downloaded', 'Superseded', or 'Removed'.
Uploading Documents to the Patient's My Health Record
Create a CDA document via one of the supplied e-Health templates in Letter Writer.
Then, within the patient's record, locate the document you wish to upload. Documents can reside on either of the Correspondence, Documents, Results or Letters tabs.
Click
 You will
be presented with a preview of the document.
You will
be presented with a preview of the document.
If you are satisfied that this is the document you wish to upload, click Send on the preview window.
The upload will commence and you will be notified upon completion. The 'My Health Record Status' and 'My Health Record Activity Date' columns within the correspondence tabs of the patient's record will indicate the selected document's My Health Record status.
Superseding Documents
A Shared Health Summary cannot be superseded.
You can only supersede a given document with the same type of document. For example, an e-Referral can only be superseded by another e-Referral.
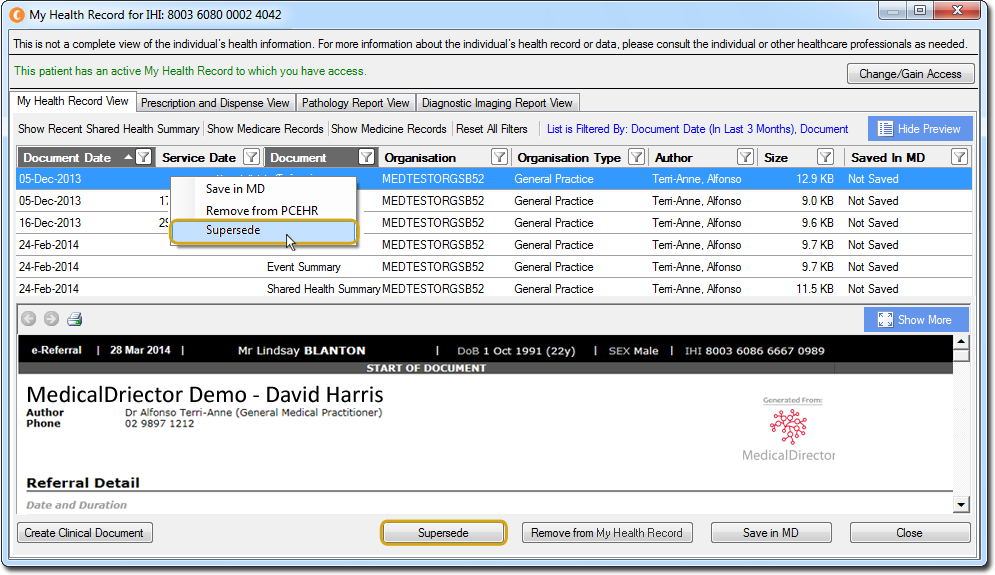
Within
the My Health Record window, locate and right-click the document
you wish to supersede, and select Supersede from the menu that
appears.
The
Select a Document window appears.

Browse through the list of available documents from your patient's record, and select the document you wish to use to replace that within My Health Record.
Click
 The document will be uploaded to My
Health Record, to replace the existing document.
The document will be uploaded to My
Health Record, to replace the existing document.
Uploading Medications to the Patient's My Health Record and NPDR
With a patient’s consent, prescriptions can be uploaded to their My Health Record. The upload occurs automatically when you print a script. Consent is typically indicated via the Enter Dose window during the prescribing process, but can also be granted/revoked afterwards by right-clicking an item on the CurrentRx tab and clicking the My Health Record Consent entry from the menu that appears.
The National Prescription and Dispense Repository (NPDR) is a subset of a patient’s My Health Record and allows for the creation of an online medication history (for both prescriptions and dispensing). Transfer of medications in this way requires you are registered for ePrescribing and have enabled eRx Script Exchange.
Prerequisites:
Practitioner is registered for ePrescribing. See ePrescribing Configuration for instructions.
My Health Record is configured correctly. See Configuring MedicalDirector Clinical for My Health Record for instructions.
Practitioner has indicated their participation in My Health Record. See below for details.
For further information regarding the NPDR, please refer to the following link:
www.ehealth.gov.au/internet/ehealth/publishing.nsf/Content/faqs-hcp-managing#anchor11
Downloading Medications from the Patient's My Health Record
Within
the patient’s record, click MyHealthRecord.

The
My Health Record window appears. Select the Prescription
and Dispense View tab. Upon selecting this tab, the patient’s
current My Health Record medications list will be retrieved and
downloaded to Clinical.
Locate
the medication you wish to save to the patient’s record, and click
![]() to display the details of the medication.
Then click the details, They will be displayed in the window.
to display the details of the medication.
Then click the details, They will be displayed in the window.

With
the details selected,
becomes available. Click this to save a copy of the medication
to the patient’s record.
Note that the medication record is only saved to the Documents
tab of the patient’s record; it is considered a document,
and cannot be used to re-prescribe from.